How research in academic labs and startups is helping boost IVF success
In 1977, UK-based Lesley and John Brown were struggling to have a baby, and their options were running out. At that time, creating an embryo outside the womb was considered a “sin” in some faiths. In vitro fertilisation (IVF) – despite multiple attempts – had not worked until then.
During one of those attempts, physiologist Robert Edwards, from the University of Cambridge, gently transferred Lesley’s egg into a Petri dish filled with John’s sperm. After a few days, embryologist Jean Purdy observed that the resultant embryo was dividing beautifully. Lesley’s gynecologist Patrick Steptoe transferred it back into her womb. Then, they waited.
On 25 July 1978, Lesley gave birth to Louise Joy Brown, the world’s first “test tube” baby. Just 67 days later, on the other side of the world, Durga, the second IVF baby was born in India, with the help of independent methods pioneered by physician Subhash Mukhopadhyay in West Bengal.
Decreasing fertility and delayed pregnancies have boosted the growth of IVF technologies in recent years. Since Louise, more than 12 million IVF babies have been born. Outside of fertility clinics, scientists and engineers in research labs are also working on cutting-edge technologies to improve IVF success rates.
When Santosh Bhargav and Ramnath Babu were doing their PhD in faculty member GK Ananthasuresh’s lab at the Department of Mechanical Engineering, IISc, they came across a surprising statistic: Current IVF success rates are only 30-40%. “WHO has declared infertility as a serious concern, and the only scientific way out of this is assisted reproductive technologies (ARTs),” says Ramnath. “[But] a lot of what is happening in ARTs is purely experience-driven; there is no first principles approach in trying to find what is the best thing to do.”
A few years ago, Santosh and Ramnath started a company called SpOvum Technologies focused on automating various procedures involved in ARTs.
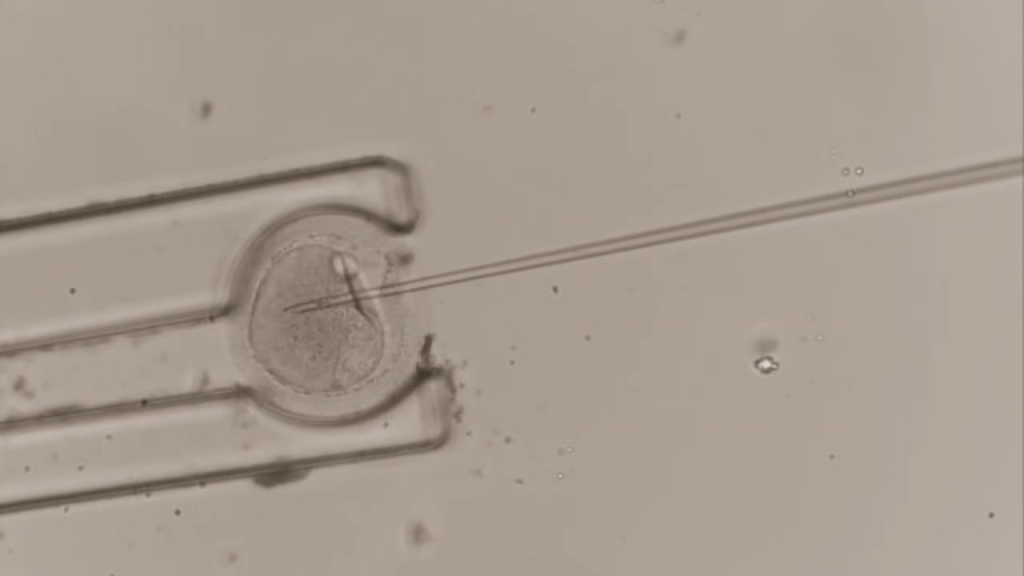
One of them is the fertilisation procedure. To increase the chances of success, clinicians nowadays inject a single, healthy sperm directly into the egg, using a method called Intracytoplasmic Sperm Injection (ICSI). But not only does the technique require highly skilled embryologists – who can handle glass micropipettes with utmost precision – it also uses technology that is now three decades old.
SpOvum came up with a novel gripper-based technique to hold the oocyte (egg cell) steady – a robotic hand with two fingers that can grip the oocyte while the sperm is being injected into it. Conventional ICSI methods lead to some oocytes getting damaged, but SpOvum’s method – called ROBO-ICSI – reduces the damage to the oocytes during sperm injection. Operating the gripper doesn’t require advanced training. SpOvum is also involved in assisting IVF clinicians all the way to a successful live birth, from using computer-aided semen analysis (CASA) systems to pick the right sperms, to developing quantitative methods for choosing the embryo with the highest chances of becoming a baby.

AI and IVF
Currently, trained embryologists subjectively decide which embryo is the best one to transfer, based on their experience of how healthy it looks. This is where Artificial intelligence (AI) can help, according to Keshav Malhotra, Vice Chairman of Embryology at the Indian Society of Assisted Reproduction. AI can rapidly analyse time-lapse videos of the developing embryo, find morphological features based on previous data, and advise embryologists on which embryo to transfer. AI tools can also help assess the quality of eggs and sperm to use.
“Recent studies have shown that the AI system is working at par with senior embryologists,” says Keshav. “In clinics with lots of embryologists and lots of [embryo transfer] cycles, AI can definitely help them standardise practices and give consistent results to their patients.”
Another issue is the rare accidental mix-up when samples get switched. Clinics usually have protocols in place to make sure that the right embryo is transferred back to the correct patient. Previously this involved a human carefully monitoring and documenting the process. Now, this “witnessing” is automated and electronic – machines simply scan codes on plasticware used in the various steps and put out warnings if they catch discrepancies.
“We are now finding out that electronic witnessing is almost 20 times faster as compared to regular witnessing and it has really streamlined the processes within the clinic itself,” Keshav says.
Keshav and Ramnath have conflicting opinions on how quickly these technologies will be adopted by clinics.
“We are trying to address a system which thinks it is in a set position; they are happy with what they are doing,” says Ramnath. “Now we are trying to tell them that ‘you should not be happy with what you’re doing because you are delivering only about 35% success rates. You have to do something more.’”
According to Keshav, however, Indian IVF clinics are at times a bit too quick to adopt new technologies. “Let’s say that I am using an experimental technology, and I am asking my patient to pay for it without knowing the long-term outcomes for that technology,” he says. “It might not be the most correct way to actually treat outpatients.”
Deepak Modi, a reproductive biologist at the ICMR-run National Institute for Research in Reproductive Health (NIRRCH), believes that after oncologists, IVF clinicians are one of the fastest adapting medical communities. But he finds it understandable that some are cautious to adopt new techniques. He draws a parallel with how users take time to adopt new phones in the market. “Everything is a bell-shaped curve, and all technologies are going to have a natural course,” he says.
In the lab

It’s not just companies like SpOvum; researchers in academic labs are also looking at ways to improve IVF.
Srimonta Gayen’s lab at the Department of Developmental Biology and Genetics (DBG), IISc, studies epigenetic changes in early embryonic development – comparing the process between natural and IVF embryos. Epigenetic changes are chemical modifications in genes; they don’t affect the gene’s sequence but could affect its function. The epigenome is easily influenced by the environmental conditions of the embryo, according to Srimonta. “In vitro, unless you give the proper conditions, you will have certain [epigenetic] changes that can also bring down the quality [of the embryo],” he explains.
His eventual goal is to ensure that early IVF embryos have similar epigenetic profiles as natural ones, which can improve their quality and increase IVF success rates. He is also studying the mechanisms behind why IVF babies skew towards males, a particularly concerning phenomenon in a country like ours.
Deepak’s lab at NIRRCH works on understanding how the embryo gets implanted in the uterus after transfer, and how to improve IVF success rates by looking at mechanisms of implantation failure. His team also developed a tool that uses machine learning to analyse genetic deletions in the Y chromosome that lead to male infertility. Using this analysis, it can predict possibilities of successful IVFs in couples with infertile men.
Srimonta and Deepak’s labs, however, are some of the very few in the country working on fundamental reproductive research. “For a country this large, we are really lacking in this particular sector,” Keshav says.
“Reproductive health is not one of the sought-after fields,” adds Deepak. “If you ask [medical] students, they say they want to study neurology or cancer.”
Keshav also points out that though IVF technology has come a long way, everyone cannot easily reap its benefits. “As far as clinical acumen and outcomes are concerned, we are probably at par with the Western world,” Keshav says. “But lots of patients from tier 2 and 3 cities might still not be able to afford IVF treatments.”
This, however, is slowly changing. According to Deepak, in the last five years, the central government has started funding affordable IVF facilities in hospitals like the All-India Institute of Medical Sciences (AIIMS). The Sikkim government, for example, offers monetary relief for couples seeking IVF treatment. Earlier, contraception for population control used to be a major national focus. “But now,” Deepak says, “the government’s investment in IVF increasing day by day.”





